












We recently found out that K2 MK-4 powder will melt into a gel/paste around ~102ºF (39ºC). Since it's summer in the northern hemisphere, we will begin shipping orders with our K2 powder in an insulated mailer with an ice pack. Sadly, we will need to charge extra for this starting March 6, 2026. Note that this extra charge includes an ice pack, an insulated mailer, and at least an upgrade to USPS priority or UPS Ground for domestic USA shipments (when you pick the "best ground shipping" option).
We will also only ship orders containing K2 powder on Monday - Wednesday trying our best to make sure it gets to you before or on Saturday. We don't want the powder potentially sitting in a delivery vehicle in the sun over the weekend.
If you're shipping destination is far away from North Carolina, please consider choosing a faster shipping service. Thank you!
We are currently shipping 1,500 mg Vitamin K2 MK-4 with the following COA (updated Mar 9, 2026):
| Serial Numbers (s/n) & Date Range Sold |
Lab Results & Info |
|---|---|
| A0450 - onward Mar 8, 2026 - onward |
Vitamin K2 MK-4 Powder
|
| See all COAs. | |
We are currently shipping 10,000 mg Vitamin K2 MK-4 with the following COA (updated Mar 2, 2026):
| Serial Numbers (s/n) & Date Range Sold |
Lab Results & Info |
|---|---|
| L0001 - L0005 Mar 2, 2026 - onward |
Vitamin K2 MK-4 Powder
|
| L0006 - onward soon |
Vitamin K2 MK-4 Powder
|
| See all COAs. | |
Note: Please keep bottle in a dark & cool place and keep the lid tightly closed (don't over-hulk it though).
Specifications (updated Feb 6, 2026, changes underlined):
- Ingredients: Vitamin K2 MK-4. That's it.
- USP grade (we are told this meets USP's specifications, however we are unable to verify this claim).
- Excipients: none.
- Source Material: Derived from geraniol, however because of the chemical reactions and transformations involved, this is considered a synthetic product (as opposed to an extract).
- County of Origin: See table above.
- Certificate of Analysis (COA) available online with every order (why the COA? | view COAs)
- Bottled in an amber glass jar for protection from UV light (why amber?)
- Bottle components country of origin: See tables above.
- Cap & bottle materials: see specification tables above.
- 1,500 mg bottle:
- dimensions: 1 x 1.8 in (25 x 46 mm) (diameter x height)
- weight w/ contents: 0.85 oz (24 g)
- 10,000 mg bottle:
- dimensions: 1.38 x 2.75 in (35 x 70 mm) (diameter x height)
- weight w/ contents: 2.15 oz (61 g)
- Expect caking/lumping/sticking of the contents as there should be no anti-caking agents. (why the "should"?)
Product changes:
Feb 19, 2024: Changed our bottle seal again, to a red tamper sticker that's more sticky.
Sept 21, 2024: Changed our bottle seal from a heat shrink wrap to a printed sticker label. The heat required to properly shrink the heat shrink wrap was causing the miniscule amount of water in the powder to evaporate out. Upon drying, the contents formed a hard "cookie" of powder.
Optional scoops:
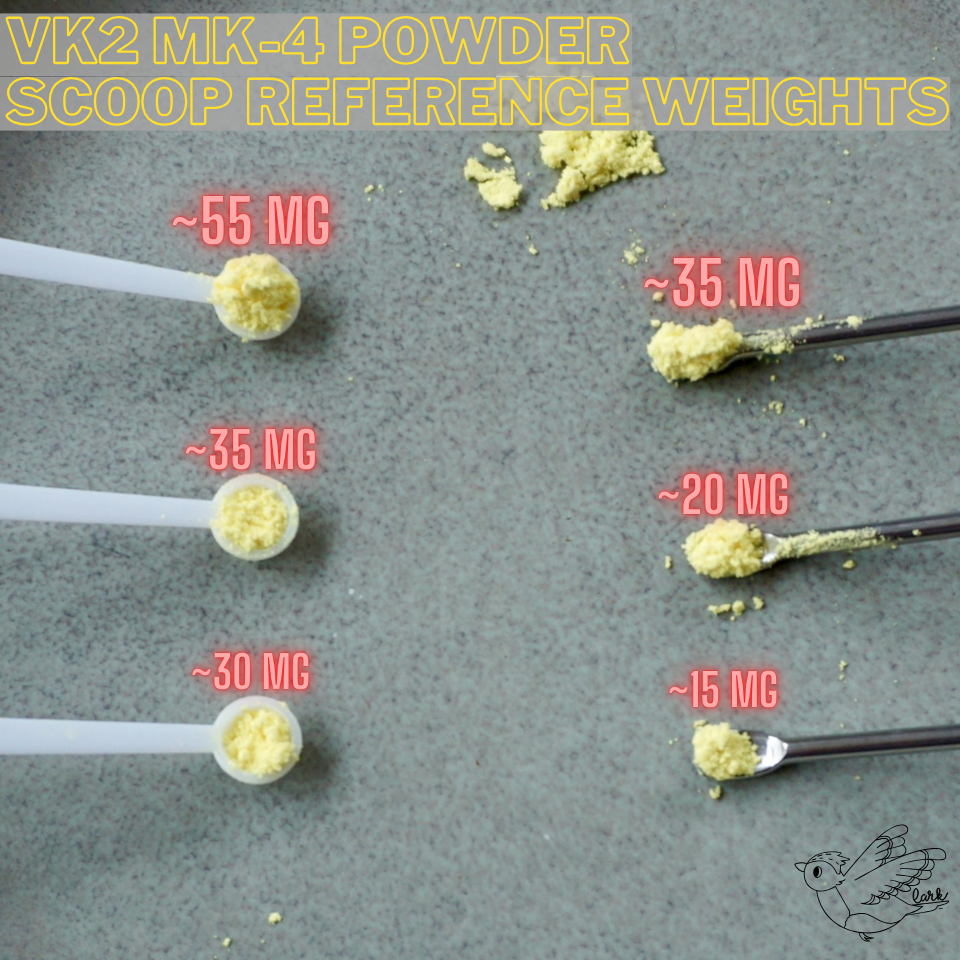
- 0.15 ml Plastic Scoop [updated Feb 16, 2026]
- Updated: holds roughly 30 - 35 mg per loose/unpacked level scoop
- New: see image for reference weight per filled scoop.
- Please wash/sterilize before use
- You may receive a white or clear scoop.
- Made in China (why China?)
- Length: 3.3 in (84 mm)
- 0.05 ml Stainless Steel (s/s) Scoop [updated Dec 9, 2024]
- Updated: holds roughly 15 - 20 mg per comfortably filled scoop
- New: see image for reference weight per filled scoop.
- The spatula tail-end can also be used as a larger scoop
- Please wash/sterilize before use
- Made in China (why China?)
- Length: 4 in (100 mm)
Oil Dilution Guidelines (updated Jan 13, 2025):
Droppers and oils vary as well as how you use the dropper. In our view, setting a standard baseline of drop weight, then using a weight ratio of VK2 to Oil makes the most sense. See our blog post about our drop experiments.
Disclosures (updated Dec 20, 2024, updates underlined):
- We use glass containers for storage and packaging, although caps and seals are usually made from silicone, plastic, rubber, or LDPE.
- We use amber colored glass or wrap clear glass to block UV rays from reaching contents.
- We store bulk powder sealed in the freezer.
- We store EVOO at room temperature (74 - 78°F or 23.3 - 25.6°C) away from sunlight.
- We steam sterilize all glass bottles, containers, caps, liners, and utensils before using them for storage or bottling using distilled water.
- We prioritize the material of
packing utensilsall containers and utensils that come into contact with product in this order: glass, ceramic, stainless steel, plastic, aluminum. - Bulk powder we receive is usually stored in an aluminum or plastic container. We immediately weigh and move it to a glass container.
- More information about our process here.
- Please also review our Terms and Conditions before placing an order.
Are we missing something that you'd like to see? Let us know!
RP on Vitamin K
"...aged cheese or well cooked greens are ordinary foods that are good sources [of vitamin k2]" - Dr. Raymond Peat, Generative Energy Podcast #31 @ 53:11
"[Protein S and C] are made under the influence of vitamin k in the liver and they are the anticoagulant factors dependent on vitamin k. So people who have excess clotting problems are sometimes told to avoid vitamin K, but if you haven't measured the proteins S and C, it might be the worst thing to do is to avoid vitamin K because vitamin K is required for the normal resolution of stimulated clotting." - Dr. Raymond Peat, Generative Energy Podcast #31 @ 53:20
"I think every other day a serving of well-cooked kale will give enough vitamin K. But the Japanese have treated osteoporosis and hardening of arteries with does of vitamin k that were 500 times the normal dietary requirement."- Dr. Raymond Peat, KMUD 2011-07-15 @ 54:43
"...it [vitamin k] is right at the center of the regulation of calcium, it protects your arteries from calcification and it allows the bones to use carbon dioxide, it carboxylates the proteins that bind calcium into the bone. So you're protecting your arteries and building your bones when you have adequate vitamin k. And both aspirin and vitamin k are known practical bone-building supplements."- Dr. Raymond Peat, KMUD 2015-07-11 @ 53:29
"It [vitamin k] puts it into your bones and keeps it from going in your arteries." - Dr. Raymond Peat, KMUD 2014-01-17 @ 52:39
"So not everyone experiences this, but if you have taken antibiotics and have a deficiency of the type of bacteria that produces vitamin k in your intestine, then you're susceptible to aspirin's knocking out of this vitamin k dependent clotting protein. So just as insurance, it's good to have a source of vitamin K in your diet." - Dr. Raymond Peat, Generative Energy Podcast #31 @ 52:44
Studies on Vitamin K
General:- Kaneki M, Hosoi T, Ouchi Y, Orimo H. Pleiotropic actions of vitamin K: protector of bone health and beyond? Nutrition. 2006 Jul-Aug;22(7-8):845-52. doi: 10.1016/j.nut.2006.05.003. PMID: 16815498. Link [pleiotropic: producing more than one effect]
- "Vitamin K is a nutrient that was originally identified as an essential factor for blood coagulation. Recently, vitamin K has emerged as a potential protector against osteoporosis, atherosclerosis, and hepatocarcinoma. Accumulated evidence indicates that subclinical non-hemostatic vitamin K deficiency in extrahepatic tissues, particularly in bone and possibly in vasculature, exists widely in the otherwise healthy adult population. Vitamins K1 and K2 have been shown to exert protective effects against osteoporosis, although it is important that the beneficial effects will be further confirmed by large-scale, randomized, clinical trials. Increasing evidence implicates a role for vitamin K in calcification of arteries and atherogenesis. Moreover, the therapeutic potential of vitamin K2 as an antihepatoma drug has recently been highlighted. Most of the new biological functions of vitamin K in bone, vasculature, and hepatoma cells are considered attributable to promotion of γ-carboxylation of glutamic acid residues in vitamin K–dependent proteins, which is shared by vitamins K1 and K2. In contrast, vitamin K2–specific, γ-carboxylation–unrelated functions have also been demonstrated. Thus, biological differences between vitamins K1 and K2 and potential involvement of γ-carboxylation–independent actions in the new roles of vitamin K remain open issues. Molecular bases of coagulation-unrelated pleiotropic actions of vitamin K and its implications in human health deserve further investigations."
- [Vitamin E and K Interactions] - Traber MG. Vitamin E and K interactions--a 50-year-old problem. Nutr Rev. 2008 Nov;66(11):624-9. doi: 10.1111/j.1753-4887.2008.00123.x. PMID: 19019024. Link
- "The mechanisms by which vitamin E interferes with vitamin K activity, especially blood clotting, are not known, but hypothetically this interference may involve metabolic pathways. Phylloquinone (K1) must be converted to menaquinone (MK-4, the most potent extrahepatic tissue vitamin K) by truncation of the K1 side chain and replacement with geranylgeranyl. Possible mechanisms for the vitamin E and K interaction include: 1) vitamin E competes for the yet undiscovered enzyme that truncates the K1 side chain; 2) vitamin E competes with K1 for the hypothetical cytochrome P450 enzyme that ω-hydroxylates the K1 side chain, thereby preventing its β-oxidation and its removal for MK-4 formation; or 3) vitamin E increases xenobiotic pathways that increase hepatic metabolism and excretion of all vitamin K forms. Currently, the pathway for K1 conversion to MK-4 is unknown, the process for regulating vitamin K metabolism to urinary excretion products is unknown, and why vitamin E supplements have such a dramatic effect, causing bleeding in some individuals and not in others, remains a mystery."
- Mishima E, Wahida A, Seibt T, Conrad M. Diverse biological functions of vitamin K: from coagulation to ferroptosis. Nat Metab. 2023 Jun;5(6):924-932. doi: 10.1038/s42255-023-00821-y. Epub 2023 Jun 19. PMID: 37337123. Link
- "Vitamin K is essential for several physiological processes, such as blood coagulation, in which it serves as a cofactor for the conversion of peptide-bound glutamate to γ-carboxyglutamate in vitamin K-dependent proteins. This process is driven by the vitamin K cycle facilitated by γ-carboxyglutamyl carboxylase, vitamin K epoxide reductase and ferroptosis suppressor protein-1, the latter of which was recently identified as the long-sought-after warfarin-resistant vitamin K reductase. In addition, vitamin K has carboxylation-independent functions. Akin to ubiquinone, vitamin K acts as an electron carrier for ATP production in some organisms and prevents ferroptosis, a type of cell death hallmarked by lipid peroxidation. In this Perspective, we provide an overview of the diverse functions of vitamin K in physiology and metabolism and, at the same time, offer a perspective on its role in ferroptosis together with ferroptosis suppressor protein-1. A comparison between vitamin K and ubiquinone, from an evolutionary perspective, may offer further insights into the manifold roles of vitamin K in biology."
- Barna M, Dunovska K, Cepova J, Werle J, Prusa R, Bjørklud G, Melichercik P, Kizek R, Klapkova E. Short-term impact of vitamin K2 supplementation on biochemical parameters and lipoprotein fractions. Electrophoresis. 2025 Feb;46(3-4):152-166. doi: 10.1002/elps.202400058. Epub 2024 Aug 2. PMID: 39091191. Link
- "This study explored the short-term effects of vitamin K2 (VK2) supplementation on biochemical parameters (vitamin D, vitamin E, vitamin A, alkaline phosphatase, calcium, phosphorus (P), magnesium, metallothionein, triglycerides, cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), and lipoprotein fractions (albumin, HDL, very low-density lipoprotein (VLDL), LDL, and chylomicrons). A short-term experiment (24 h, six probands) was performed to track changes in VK2 levels after a single-dose intake (360 µg/day). Liquid chromatography–tandem mass spectrometry was used to monitor vitamin K levels (menaquinone-4 (MK-4), menaquinone-7 (MK-7), and vitamin K1 [VK1]) with a limit of detection of 1.9 pg/mL for VK1 and 3.8 pg/mL for the two forms of VK2. Results showed that MK-7 levels significantly increased within 2–6 h post-administration and then gradually declined. MK-4 levels were initially low, showing a slight increase, whereas VK1 levels rose initially and then decreased. Biochemical analyses indicated no significant changes in sodium, chloride, potassium, calcium, magnesium, albumin, or total protein levels. A transient increase in P was observed, peaking at 12 h before returning to baseline. Agarose gel electrophoresis of lipoprotein fractions revealed distinct chylomicron bands and variations in VLDL and HDL mobility, influenced by dietary lipids and VK2 supplementation. These findings suggest effective absorption and metabolism of MK-7 with potential implications for bone metabolism and cardiovascular health."
- Bus K, Szterk A. Relationship between Structure and Biological Activity of Various Vitamin K Forms. Foods. 2021 Dec 17;10(12):3136. doi: 10.3390/foods10123136. PMID: 34945687; PMCID: PMC8701896. Link
- "Vitamin K is involved many biological processes, such as the regulation of blood coagulation, prevention of vascular calcification, bone metabolism and modulation of cell proliferation. Menaquinones (MK) and phylloquinone vary in biological activity, showing different bioavailability, half-life and transport mechanisms. Vitamin K1 and MK-4 remain present in the plasma for 8-24 h, whereas long-chain menaquinones can be detected up to 96 h after administration. Geometric structure is also an important factor that conditions their properties. Cis-phylloquinone shows nearly no biological activity. An equivalent study for menaquinone is not available. The effective dose to decrease uncarboxylated osteocalcin was six times lower for MK-7 than for MK-4. Similarly, MK-7 affected blood coagulation system at dose three to four times lower than vitamin K1. Both vitamin K1 and MK-7 inhibited the decline in bone mineral density, however benefits for the occurrence of cardiovascular diseases have been observed only for long-chain menaquinones. There are currently no guidelines for the recommended doses and forms of vitamin K in the prevention of osteoporosis, atherosclerosis and other cardiovascular disorders. Due to the presence of isomers with unknown biological properties in some dietary supplements, quality and safety of that products may be questioned."
- The amount of vitamin K was determined in a series of plant organs by the curative technique.
The richest sources were green leaves of different kinds, chestnut leaves being the most potent among the species examined.
During the withering of green leaves the amount of vitamin K was not much altered. Leaves which had large yellow areas alternating with green ones contained approximately as much vitamin K in the yellow areas as in the green. The vitamin K content of flowers, roots and seeds was found to be much less than that of green leaves; mangold root was a particularly poor source.
Certain lower plants appeared to be poorer sources than higher plants.
An experiment with germinating peas showed that whereas there was an abundant synthesis of the vitamin in peas grown in the light, synthesis in peas grown in the dark occurred to a very limited extent.
- [Maternal Vitamin K Supplementation and Breastfeeding Infants Vitamin K Status] - Nishiguchi T, Yamashita M, Maeda M, Matsuyama K, Kobayashi T, Kanayama N, Terao T. Improvement of vitamin K status of breastfeeding infants with maternal supplement of vitamin K2 (MK40). Semin Thromb Hemost. 2002 Dec;28(6):533-8. doi: 10.1055/s-2002-36697. PMID: 12536346. Link
- "The present study is aimed at evaluating the efficacy of maternal vitamin K2 supplementation on the vitamin K status of newborn infants using the measurement of des-gamma-carboxyprothrombin (PIVKA-II [protein induced by vitamin K absence]) and the hepaplastin test (HPT). PIVKA-II and HPT were measured at the 1st month of age in two groups: 31 infants with maternal vitamin K supplementation (15 mg/d Menatetrenone since the 14th day after parturition) (group 1) and 46 without maternal supplementation (group 2). All infants received vitamin K2 syrup twice within the 1st week of life. The PIVKA-II levels of 31 infants (group 1) were 23.6 mAU/mL (standard deviation [SD] 5.8), showing extremely low levels, and close to healthy adult levels, with a smaller deviation than what was seen in group 2. The levels of the 46 infants in group 2 were 27.8 (SD 16.0). This does not differ significantly from group 1, but a small number of infants showed a modestly high level in PIVKA-II. There also was no significant difference between the two groups in the HPT. These data would indicate that maternal vitamin K supplementation can maintain the vitamin K status throughout the late neonatal period and prevent an onset of vitamin K-deficient hemorrhage."
- Jun Iwamoto, Tsuyoshi Takeda, Shoichi Ichimura, Effect of menatetrenone on bone mineral density and incidence of vertebral fractures in postmenopausal women with osteoporosis: a comparison with the effect of etidronate, Journal of Orthopaedic Science, Volume 6, Issue 6, 2001, Pages 487-492, ISSN 0949-2658, https://doi.org/10.1007/s007760100002 Link
- "The purpose of the present study was to compare the effects of etidronate and menatetrenone on bone mineral density (BMD) and the incidence of vertebral fractures in postmenopausal women with osteoporosis. Seventy-two osteoporotic women, more than 5 years after menopause, 53–78 years of age, were randomly divided into three administration groups: E group; intermittent cyclical etidronate (200 mg/day, 14 days per 3 months; n = 25); M group; menatetrenone (45 mg/day, daily; n = 23); and C group (control); calcium lactate (2 g/day, daily; n = 24). Forearm BMD was measured by dual-energy X-ray absorptiometry at 0, 6, 12, 18, and 24 months after the treatment started. There were no significant differences in age, body mass index, years since menopause, and initial BMD among the three groups. One-way analysis of variance (ANOVA) with repeated measurements showed a significant decrease in BMD in the C group (P < 0.0001). Two-way ANOVA with repeated measurements showed a significant increase in BMD in the M group compared with that in the C group (P < 0.0001), and a significant increase in BMD in the E group compared with that in the C and M groups (P < 0.0001 and P < 0.01, respectively). The indices of new vertebral fractures/1000 patient-years in the E and M groups were significantly higher than that in the C group (χ2 = 47.7; P < 0.0001 and χ2 = 42.4; P < 0.0001, respectively), and did not differ significantly between the E and M groups. The present preliminary study provides evidence to suggest that, despite the lower increase in BMD produced by menatetrenone, this agent, as well as etidronate, may have the potential to reduce osteoporotic vertebral fractures in postmenopausal women with osteoporosis."
- Iwamoto J. Vitamin K₂ therapy for postmenopausal osteoporosis. Nutrients. 2014 May 16;6(5):1971-80. doi: 10.3390/nu6051971. PMID: 24841104; PMCID: PMC4042573. Link
- "Vitamin K may play an important role in the prevention of fractures in postmenopausal women with osteoporosis. Menatetrenone is the brand name of a synthetic vitamin K2 that is chemically identical to menaquinone-4. The present review study aimed to clarify the effect of menatetrenone on the skeleton in postmenopausal women with osteoporosis, by reviewing the results of randomized controlled trials (RCTs) in the literature. RCTs that investigated the effect of menatetrenone on bone mineral density (BMD), measured by dual-energy X-ray absorptiometry and fracture incidence in postmenopausal women with osteoporosis, were identified by a PubMed search for literature published in English. Eight studies met the criteria for RCTs. Small RCTs showed that menatetrenone monotherapy decreased serum undercarboxylated osteocalcin (ucOC) concentrations, modestly increased lumbar spine BMD, and reduced the incidence of fractures (mainly vertebral fracture), and that combined alendronate and menatetrenone therapy enhanced the decrease in serum ucOC concentrations and further increased femoral neck BMD. This review of the literature revealed positive evidence for the effects of menatetrenone monotherapy on fracture incidence in postmenopausal women with osteoporosis. Further studies are required to clarify the efficacy of menatetrenone in combination with bisphosphonates against fractures in postmenopausal women with osteoporosis."
- Cerqua C, Casarin A, Pierrel F, Vazquez Fonseca L, Viola G, Salviati L, Trevisson E. Vitamin K2 cannot substitute Coenzyme Q10 as electron carrier in the mitochondrial respiratory chain of mammalian cells. Sci Rep. 2019 Apr 25;9(1):6553. doi: 10.1038/s41598-019-43014-y. PMID: 31024065; PMCID: PMC6484000. Link
- "Coenzyme Q10 (CoQ10) deficiencies are a group of heterogeneous conditions that respond to ubiquinone administration if treated soon after the onset of symptoms. However, this treatment is only partially effective due to its poor bioavailability. We tested whether vitamin K2, which was reported to act as a mitochondrial electron carrier in D. melanogaster, could mimic ubiquinone function in human CoQ10 deficient cell lines, and in yeast carrying mutations in genes required for coenzyme Q6 (CoQ6) biosynthesis. We found that vitamin K2, despite entering into mitochondria, restored neither electron flow in the respiratory chain, nor ATP synthesis. Conversely, coenzyme Q4 (CoQ4), an analog of CoQ10 with a shorter isoprenoid side chain, could efficiently substitute its function. Given its better solubility, CoQ4 could represent an alternative to CoQ10 in patients with both primary and secondary CoQ10 deficiencies."
- Xu C, Cunqing Y, Chun G, Min W, Jun L, Xueyun H, Jiaxin F, Li S, Cheng A, Guijian L, Fengxiang S, Bo P. The relationship between serum vitamin K concentration and coronary artery calcification in middle-aged and elderly people. Clin Chim Acta. 2022 Jun 1;531:325-330. doi: 10.1016/j.cca.2022.04.1001. Epub 2022 May 2. PMID: 35504322. Link
- "Background: Vitamin K is involved in the formation of coronary artery calcification which is an independent predictor of coronary heart disease. This study aims to explore the association between coronary artery calcification score and serum concentrations of vitamin K1, menaquinone-4 (MK-4) and menaquinone-7 (MK-7) in middle-aged and elderly Chinese population.
Methods: A total of 116 patients who underwent CT coronary angiography were consecutively enrolled. Serum concentrations of vitamin K1, MK-4 and MK-7 were determined by high performance liquid chromatography tandem mass spectrometry. The relationships between coronary artery calcification score and serum vitamin K concentrations were analyzed.
Results: Significantly lower serum vitamin K1 concentration was found in the patients with CACS > 400, comparing with the other CACS categories, respectively. Log (CACS + 1) was significantly higher in MK-4 < 0.05 ng/ml group compared with MK-4 ≥ 0.05 ng/ml group [2.03(0.21, 2.58) vs 1.31(0.00, 2.19), P < 0.05]. In subjects with established coronary calcification (defined as CACS > 10), vitamin K1 was found to be an independent factor contributing to higher CACS (r = -0.288, P = 0.013).
Conclusions: In this retrospective analysis, serum vitamin K1 and MK-4 concentrations were significantly lower in middle-aged and elderly cohorts with increasing calcification scores. The significant effect of vitamin K1 on CACS was only found in individuals who already had calcification. Whether the detection of circulating vitamin K in patients with preexisting coronary calcification could guide vitamin K supplementation needs further exploration."
- "Background: Vitamin K is involved in the formation of coronary artery calcification which is an independent predictor of coronary heart disease. This study aims to explore the association between coronary artery calcification score and serum concentrations of vitamin K1, menaquinone-4 (MK-4) and menaquinone-7 (MK-7) in middle-aged and elderly Chinese population.
- [Sponsored by Nattopharma ASA, a producer of MK-7] - Knapen MH, Drummen NE, Smit E, Vermeer C, Theuwissen E. Three-year low-dose menaquinone-7 supplementation helps decrease bone loss in healthy postmenopausal women. Osteoporos Int. 2013 Sep;24(9):2499-507. doi: 10.1007/s00198-013-2325-6. Epub 2013 Mar 23. PMID: 23525894. Link
- "We have investigated whether low-dose vitamin K2 supplements (menaquinone-7, MK-7) could beneficially affect bone health. Next to an improved vitamin K status, MK-7 supplementation significantly decreased the age-related decline in bone mineral density and bone strength. Low-dose MK-7 supplements may therefore help postmenopausal women prevent bone loss.
Introduction: Despite contradictory data on vitamin K supplementation and bone health, the European Food Safety Authorities (EFSA) accepted the health claim on vitamin K's role in maintenance of normal bone. In line with EFSA's opinion, we showed that 3-year high-dose vitamin K1 (phylloquinone) and K2 (short-chain menaquinone-4) supplementation improved bone health after menopause. Because of the longer half-life and greater potency of the long-chain MK-7, we have extended these investigations by measuring the effect of low-dose MK-7 supplementation on bone health.
Methods: Healthy postmenopausal women (n = 244) received for 3 years placebo or MK-7 (180 μg MK-7/day) capsules. Bone mineral density of lumbar spine, total hip, and femoral neck was measured by DXA; bone strength indices of the femoral neck were calculated. Vertebral fracture assessment was performed by DXA and used as measure for vertebral fractures. Circulating uncarboxylated osteocalcin (ucOC) and carboxylated OC (cOC) were measured; the ucOC/cOC ratio served as marker of vitamin K status. Measurements occurred at baseline and after 1, 2, and 3 years of treatment.
Results: MK-7 intake significantly improved vitamin K status and decreased the age-related decline in BMC and BMD at the lumbar spine and femoral neck, but not at the total hip. Bone strength was also favorably affected by MK-7. MK-7 significantly decreased the loss in vertebral height of the lower thoracic region at the mid-site of the vertebrae.
Conclusions: MK-7 supplements may help postmenopausal women to prevent bone loss. Whether these results can be extrapolated to other populations, e.g., children and men, needs further investigation."
- "We have investigated whether low-dose vitamin K2 supplements (menaquinone-7, MK-7) could beneficially affect bone health. Next to an improved vitamin K status, MK-7 supplementation significantly decreased the age-related decline in bone mineral density and bone strength. Low-dose MK-7 supplements may therefore help postmenopausal women prevent bone loss.
- [Sato, T works for J-OIL MILLS, INC, a producer of MK-7 ] - Sato T, Schurgers LJ, Uenishi K. Comparison of menaquinone-4 and menaquinone-7 bioavailability in healthy women. Nutr J. 2012 Nov 12;11:93. doi: 10.1186/1475-2891-11-93. PMID: 23140417; PMCID: PMC3502319. Link
- "Background: Vitamin K₂ contributes to bone and cardiovascular health. Therefore, two vitamin K₂ homologues, menaquinone-4 (MK-4) and menaquinone-7 (MK-7), have been used as nutrients by the food industry and as nutritional supplements to support bone and cardiovascular health. However, little is known about the bioavailability of nutritional MK-4. To investigate MK-4 and MK-7 bioavailability, nutritional doses were administered to healthy Japanese women.
Findings: Single dose administration of MK-4 (420 μg; 945 nmol) or MK-7 (420 μg; 647 nmol) was given in the morning together with standardized breakfast. MK-7 was well absorbed and reached maximal serum level at 6 h after intake and was detected up to 48 h after intake. MK-4 was not detectable in the serum of all subjects at any time point. Consecutive administration of MK-4 (60 μg; 135 nmol) or MK-7 (60 μg; 92 nmol) for 7 days demonstrated that MK-4 supplementation did not increase serum MK-4 levels. However, consecutive administration of MK-7 increased serum MK-7 levels significantly in all subjects.
Conclusions: We conclude that MK-4 present in food does not contribute to the vitamin K status as measured by serum vitamin K levels. MK-7, however significantly increases serum MK-7 levels and therefore may be of particular importance for extrahepatic tissues."
- "Background: Vitamin K₂ contributes to bone and cardiovascular health. Therefore, two vitamin K₂ homologues, menaquinone-4 (MK-4) and menaquinone-7 (MK-7), have been used as nutrients by the food industry and as nutritional supplements to support bone and cardiovascular health. However, little is known about the bioavailability of nutritional MK-4. To investigate MK-4 and MK-7 bioavailability, nutritional doses were administered to healthy Japanese women.
- Kaesler N, Schreibing F, Speer T, Puente-Secades S, Rapp N, Drechsler C, Kabgani N, Kuppe C, Boor P, Jankowski V, Schurgers L, Kramann R, Floege J. Altered vitamin K biodistribution and metabolism in experimental and human chronic kidney disease. Kidney Int. 2022 Feb;101(2):338-348. doi: 10.1016/j.kint.2021.10.029. Epub 2021 Nov 11. PMID: 34774554. Link
- "Chronic kidney disease (CKD) is accompanied with extensive cardiovascular calcification, in part correlating with functional vitamin K deficiency. Here, we sought to determine causes for vitamin K deficiency beyond reduced dietary intake. Initially, vitamin K uptake and distribution into circulating lipoproteins after a single administration of vitamin K1 plus K2 (menaquinone 4 and menaquinone 7, respectively) was determined in patients on dialysis therapy and healthy individuals. The patients incorporated very little menaquinone 7 but more menaquinone 4 into high density lipoprotein (HDL) and low-density lipoprotein particles than did healthy individuals. In contrast to healthy persons, HDL particles from the patients could not be spiked with menaquinone 7 in vitro and HDL uptake was diminished in osteoblasts. A reduced carboxylation activity (low vitamin K activity) of uremic HDL particles spiked with menaquinone 7 vs. that of controls was confirmed in a bioassay using human primary vascular smooth muscle cells. Kidney menaquinone 4 tissue levels were reduced in 5/6-nephrectomized versus sham-operated C57BL/6 mice after four weeks of a vitamin K rich diet. From the analyzed enzymes involved in vitamin K metabolism, kidney HMG-CoA reductase protein was reduced in both rats and patients with CKD. In a trial on the efficacy and safety of atorvastatin in 1051 patients with type 2 diabetes receiving dialysis therapy, no pronounced vitamin K deficiency was noted. However, the highest levels of PIVKA-II (biomarker of subclinical vitamin K deficiency) were noted when a statin was combined with a proton pump inhibitor. Thus, profound disturbances in lipoprotein mediated vitamin K transport and metabolism in uremia suggest that menaquinone 7 supplementation to patients on dialysis therapy has reduced efficacy."
17 Reviews Hide Reviews Show Reviews
-
Vitamin K2 Mk-4 Powder
Amazing quality product! Amazing kind client service! Amazing wonderful cuddly art drawings! Only Amazing human beings can create this! I am grateful!
-
K2 MK4
Great product, affordable, transparent company. Nothing beats this in terms of price and quality.
-
K2 powder
Great to be able to self select your dose with the powder
-
Vitamin K2. mK4
Have a ton of confidence in Richard’s products!
-
Perfect
One of, if not the best product on the market
-
Vitamin K2 MK-4
Best vitamin K2 on the market. In my experience, it lowers estrogen more effectively than any other K2 supplement that I have tried.
-
High Quality, Cheaper Than Bulgarian Product
100% Peaty. Will be buying this product regularly.
-
Lark’s Vitamin K2 is of exceptional quality as it is stated on the website
Besides the best quality of Lark’s product, The service is of exceptional quality, Products are delivered within days and Queries are resolved over email within 24hrs
-
Loving this MK-4
I prefer the powder form of K2, and being able to measure and mix in the carrier of my choice. Typically I take it with pastured dairy (cottage cheese, cream or yogurt) or organic EVOO. Lark Supply K2 powder is high purity, and their customer service is outstanding!


